Screening of 1003 whole blood samples
from febrile patients in Mbeya, Tanzania,
for the presence of Relapsing Fever Borrelia using real-time PCR
Christoph Lütke Daldrupa, b, Volker Fingerlec, Anna-Cathrine Neumanna, b, d, Gabriele Margosc, Michael Hoelschera, d, Norbert Heinricha, d, Gerhard Doblere, Andreas Wiesera, b, d
a Division of Infectious Diseases and Tropical Medicine, University Hospital Munich
b Chair of Medical Microbiology and Hospital Epidemiology, Faculty of Medicine, Max von Pettenkofer Institute, LMU, Munich, Germany
c National Reference Center for Borrelia, Bavarian Health and Food Safety Authority, Oberschleissheim, Germany
d German Center for Infection Research (DZIF), Partner Site Munich, 80802 Munich, Germany
e Bundeswehr Institute of Microbiology, Department Virology and Intracellular Agents
Background
Relapsing fevers are vector borne diseases caused by bacteria of the genus Borrelia. Main vector are soft ticks of the genus Ornithodoros. The clinical course is characterized by recurrent episodes of fever. Epidemiologically relapsing fevers are more common in settings with limited resources; they rarely occur in central Europe.
There are two main groups of relapsing fever, Louse borne relapsing fever (LBRF), caused by Borrelia recurrentis, is transmitted by the body louse; it is characterized by high mortality rates and epidemic occurrences. Tick borne relapsing fever (TBRF) is mainly transmitted by soft ticks and caused by different related Borrelia species. TBRF can be found in certain geographical areas epidemically and occurs sporadically in patients. The clinical course is mostly less severe, lethality is low. Reports about the prevalence of TBRF vary considerably in the literature. It is generally assumed that the burden of disease is underestimated due to the lack of sensitive detection in patient material.
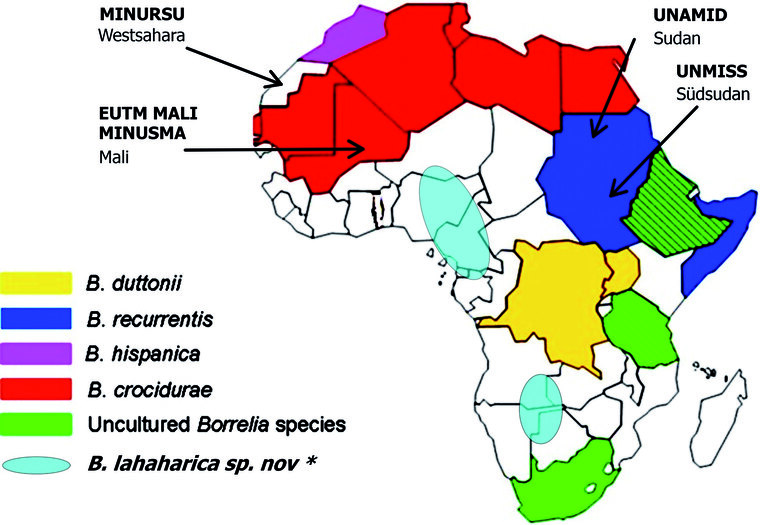
Fig 1: Endemic occurence of different Borrelia species in Africa (map taken from Elbir H, Raoult D, Drancourt M: Relapsing fever Borreliae in Africa. AM J TropMed 2013; 89(2): 288-292); * first description by Fingerle V, Pritsch M, Wächtler M et al.: Candidatus Borrelia kalaharica Detected from a Febrile Traveller Returning to Germany from Vacation in Southern Africa. PLOS Neglected Tropical Diseases 2016; 10(3): e0004599.)
Material and methods
In this study, 1.003 blood samples from people of the Mbeya region (Tanzania), which were collected during the HOMA trial were investigated for the prevalence of Borrelia DNA. Therefore, freshly frozen whole blood samples of acute febrile patients were extracted using a robotic platform and investigated for the presence of Borrelia DNA with two different and newly validated real-time PCR protocols.
The protocols were validated with enumerated Borrelia cultures, as well as extracted positive blood samples to reach a sensitivity of 102-101 DNA copies/5µl. Controls included T/L-BRF strains from B. miyamatoi, B. hermsii and B. recurrentis. Lyme group Borrelia were also detected.
One protocol was based on SYBR green, the second on TaqMan probes, both using a different set of primers. Similar studies used this approach successfully to detect Borrelia in the blood of patients [3].

Fig. 2: Microscopy of borreliae (red circle) in a blood smear
Results
Within this study however, no Borrelia could be detected, probably due to regional peculiarities. It may be a highly unlikely sporadically occurring disease which is of less importance given the overall disease burden. The patient cohort was selected to be regionally as well as socio-economically diverse. A significant proportion of the study participants were rural inhabitants with livestock keeping.
Discussion and conclusions
This is the first cohort of acute febrile patients in the Mbeya region, which has been screened for relapsing fever Borrelia. Within the sample, no relapsing fever cases could be found. Thus, the disease seems to be absent or present only in very small numbers in the population.
Nevertheless, many different human pathogenic borrelia species can be found in Africa. It must expected that soldiers and locals get in contact with soft ticks and become infected by tick borne relapsing fever. Mainly soldiers taking cover or sleeping in primitive shelters are at risk. Aggressive feeding behaviour and drought resistance make soft ticks effective vectors. Availibility of valid diagnostic tools and medical personnel thinking of TBRF in case of a febtile illness is evident for deployed forces.
References
- Cutler SJ, Idirs JM, Ahmed AO, Elelu N: Ornithodoros savignyi, the Tick Vector of "Candidatus Borrelia kalaharica" in Nigeria. J Clin Microbiol 2018; 56(9): e00532-18. mehr lesen
- Elbir H, Raoult D Drancourt M: Relapsing fever borreliae in Africa. The American journal of tropical medicine and hygiene 2013; 89(2): 288-292. mehr lesen
- Melkert P, Kahema L, van der Velden J, van Roosmalen J: Relapsind fever, a dissapearing cause of fever and maternal death in Sengerema, Tanzania, East Africa. East Afr Med J 2013; 90(4): 137-141. mehr lesen
Manuskriptdaten
Zitierweise
Lüttke Daldrup C, Fingerle V, Neumann AC, Margos G, Hoelscher M, Heinrich N, Dobler G, Wieser G: Screening of 1003 whole blood samples from febrile patients in Mbeya, Tanzania, for the presence of Relapsing Fever Borrelia using real-time PCR (Poste-Abstract). WMM 2019; 64(1): 30-31.
Für die Verfasser
Leutnant SanOA Christoph Lütke Daldrup
Sanitätsakademie der Bundeswehr
Neuherbergstr. 1, 80937 München
E-Mail: christoph.luetke.daldrup@san-netz.de
Der Beitrag wurde als Poster beim 50. Jahreskongress der Deutschen Gesellschaft für Wehrmedizin und Wehrpharmazie e. V. (Leipzig, 10.-12. Oktober 2019) präsentiert und belegte beim Posterwettbewerb der Gesundheitseinrichtungen den ersten Platz.