
ÜBERSICHTSARBEIT
Vitamin D deficiency: An often underestimated risk
Emanuel Vitsa , Markus Staudta , Maike Berresheima , Ulrich Rohdea , Thomas Egerb , Christoph Bickelc , Dieter Leyka,d
a Bundeswehr Institute for Preventive Medicine, Division A Health and Fitness Promotion, Andernach/Koblenz
b Bundeswehr Central Hospital Koblenz, Department XXIII Dentistry, Koblenz
c Bundeswehr Central Hospital Koblenz, Department I Internal medicine, Koblenz
d German Sport University Colgone, Research Group Epidmemiology of Performance, Colgone
Summary
Vitamin D does not only play an essential role in calcium and bone metabolism, but also has numerous preventive and curative effects in other organ systems. However, literature reviews show large differences regarding minimum vitamin D levels and vitamin D supplementation. In this study, a systematic literature search was conducted to determine the background for these divergent statements and to examine whether vitamin D supplementation is recommended for soldiers.
Various professional societies currently assume a vitamin D deficiency if serum vitamin D levels (calcidiol, 25-hydroxyvitamin D3; 25(OH)D3) are below 20 ng/ml (= 50 nmol/l). Epidemiological studies, however, hint at higher levels for normal serum concentrations: Vitamin D serum levels of 30 ng/ml (= 75 nmol/l) are associated with lower cardiometabolic and inflammatory biomarker levels. Newer studies provide supportive evidence that the different effects of vitamin D in the organism are concentration- and tissue related. Vitamin D levels in indigenous ethnic groups living close to the equator are markedly above 40 ng/ml (> 100 nmol/ml).
Roughly 60 % of the German population has an undersupply of vitamin D. More than 80 % of men and 90 % of women do not reach the recommended daily vitamin D intake. Due to the low UV indices during the winter half year In Germany, vitamin D production in the skin (the actual main source) is insufficient. There is an increased risk of vitamin D deficiency in numerous population groups, which is further increased by staying behind window glass, in closed rooms, etc.
There are further restrictions of endogenous vitamin D production in military due to wearing of long-sleeved uniforms, protective equipment, and headgear. In a group of German Air Force personnel (> 2,000 persons) vitamin D deficiency was found in over 70%. In view of the new findings and the special circumstances in the military sector, targeted supplementation of vitamin D in female and male soldiers is clearly recommended.
Key Words: supplementation, military; prevention; deficency; risk factors
Introduction
The interest in vitamin D has increased considerably in the last 20 years. Only in 2020, more than 5,100 scientific publications were released to PubMed (PubMed query as of March 8, 2021). There is also more media coverage of vitamin D. Reasons for the increased attention are new findings on vitamin D effects that go far beyond the known endocrine control of calcium homeostasis and bone metabolism [ 4][15][22][31]. It is now well established that vitamin D has additional autocrine and paracrine effects in most tissues. The activated and membrane-permeable steroid hormone calcitriol (1,25- dihydroxycholecalciferol; 1,25(OH)2 D3 ) has multiple influences on, among others, gene expression [22][58], and epigenetics [14][15][71].
Lowered vitamin D levels have been reported in connection with numerous diseases (see Table 1 ). According to meta-analyses, vitamin D deficiency alone is a risk factor for various diseases in several organ systems. The Umbrella Review published in 2020 [ 44], for example, shows positive effects of a vitamin D supplementation in the primary prevention of acute respiratory tract infections, as well as in dementia, cognitive decline, and depression. Among others, curative effects exist in patients with asthma and COPD [ 7][44]. The outcomes of dental periodontitis and peri-implantitis therapy show more favorable treatment results [42], and there is also evidence of a positive vitamin D influence in SARS- CoV-2 infections [20][36]. In Table 2 diseases showing positive effects from Vitamin D treatment are listed.
Table 1: Diseases and medication frequently associated with low vitamin D levels (according to: [4][9][21][54][59][61][70][71]).
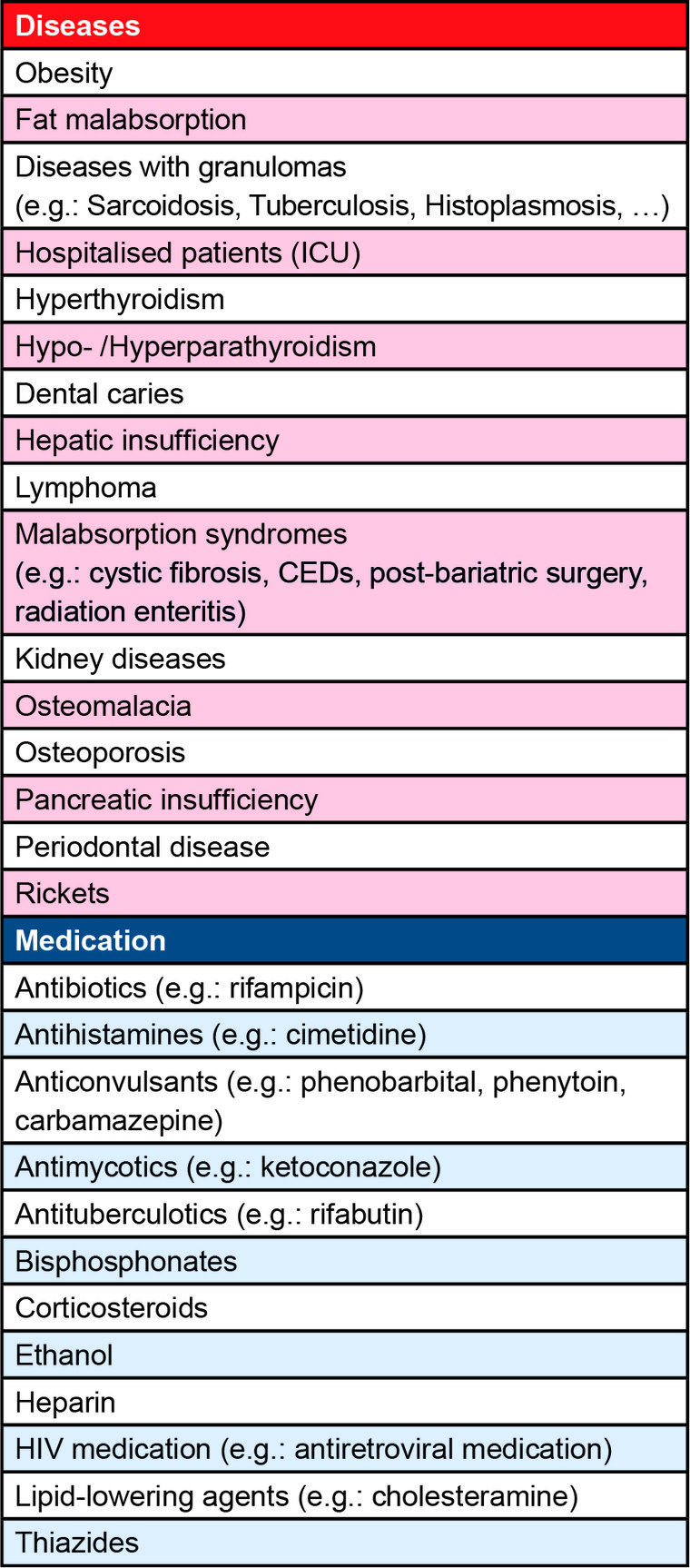
Table 2: Diseases with confirmed positive effects of vitamin D administration.
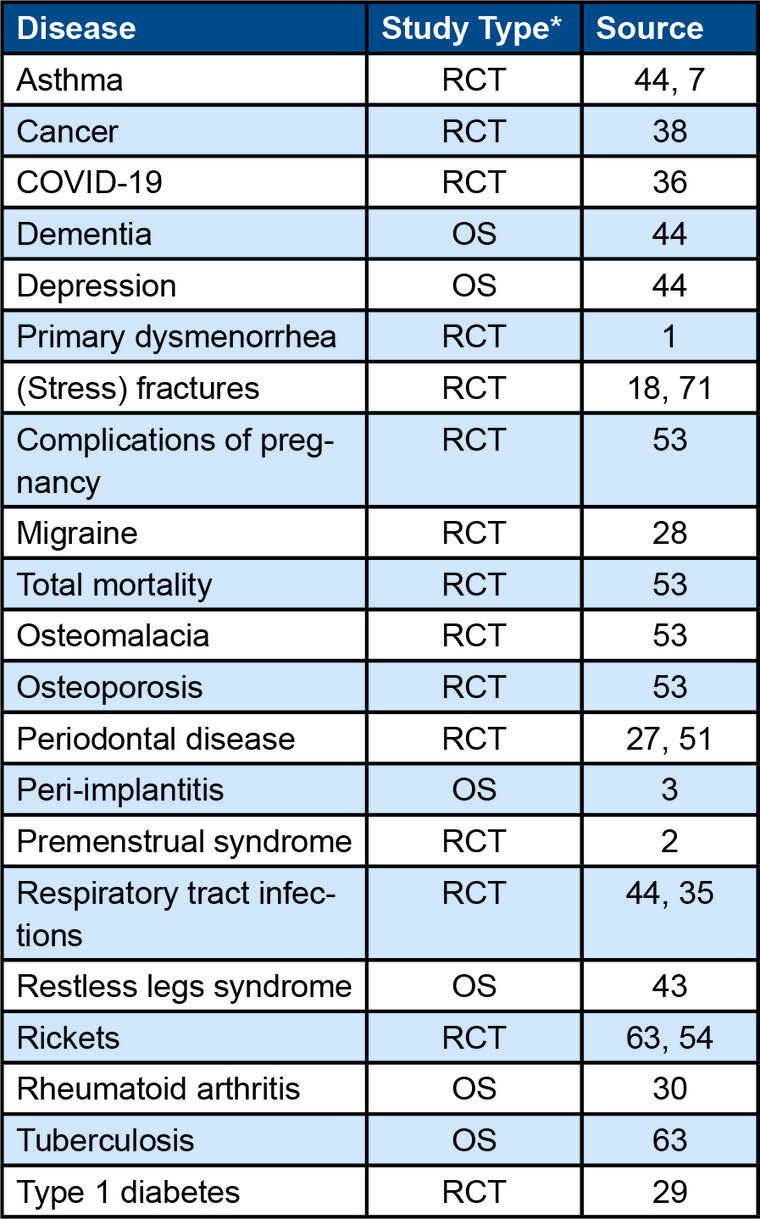
* RCT = Randomized Controlled Study, OS = Observational Study/Beobachtungsstudie
Recently published RCTs showed a 13 % reduction decrease in cancer mortality through vitamin D administration [38], which would lead to savings of more than 250 million euros in Germany alone [49].
While the multitude of vitamin D effects are scientifically undisputed by now, there is only a partial consensus regarding vitamin D supply [71]. Thus, recommendations differ considerably with regard to vitamin D levels, actual vitamin D requirements, and the need of supplementation [53]. In literature, vitamin D serum levels are listed in ng/ml or nmol/l ( 1 ng/ml = 2.5 nmol/l), while the required amounts of vitamin D are given in IU and µg ( 40 IU = 1 µg).
The recommended minimum level of calcidiol (25-hydroxyvitamin D3 ; 25(OH)D3 )) varies from 10 ng/ml (= 25 nmol/l; [63]) to 30 ng /ml (= 75 nmol/l; [32]) depending on the professional society. The D-A-CH Nutrition Society (Germany: Deutsche Gesellschaft für Ernährung (DGE), Austria (ÖGE), Switzerland (SGE, SVE)) recommend minimum levels of ≥ 20 ng/ml (≥ 50 nmol/l) [48]. Much higher minimum levels (40 ng/ml–60 ng/ml (= 100 nmol/l–150 nmol/l)) are mentioned by the “ VitaminD Society” [67], among others.
In this review, we present the background for the deviating reference ranges and recommendations for the normal vitamin D requirement. In addition, usefulness of vitamin D supplementation for soldiers is assessed.
Methodology
A systematic literature search according to the “preferred reporting items for systematic review and meta-analysis” (PRISMA recommendations) was conducted in the PubMed database (https://pubmed.ncbi.nlm.nih.gov/) in the period from 02/01/2021 to 03/23/2021. The search term “Vitamin D” was used to search for systematic reviews published in German or English in the last 10 years. In addition to an analysis of the cited literature, a hand search was carried out using the terms “Vitamin D & physiology”, “Vitamin D & recommendation”, “ Vitamin D & status”, “Vitamin D & Germany”, “Vitamin D & sport”, “Vitamin D & Armed Forces”, and “Vitamin D & Bundeswehr” (time-period: last 10 years). Current articles were prioritized and other articles were screened for substantially contradictory opinions. Studies on adolescents (under 18 years), pregnant women, and seniors (over 65 years) as well as clinical reviews on specific diseases were excluded. Figure 1 shows the PRISMA flow chart including literature selection. From a total of 1262 articles, 168 studies were evaluated in the present publication.
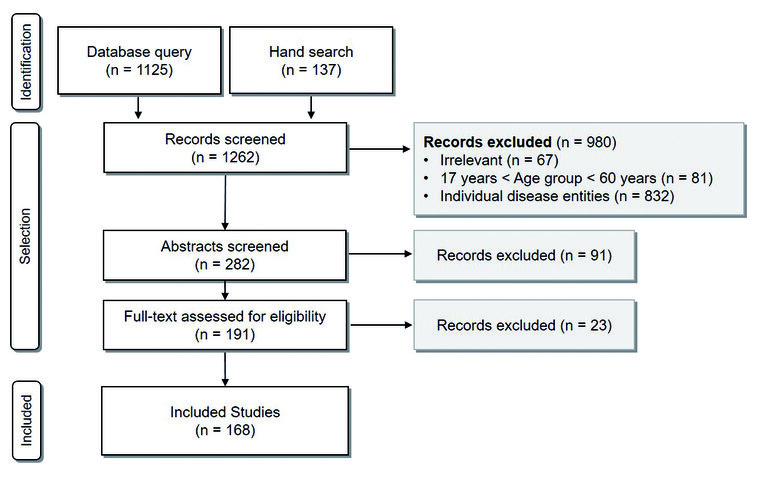
Figure 1: PRISMA flow chart of the literature search for systematic reviews; search term: “Vitamin D”, search timeframe: last 10 years
Results
Vitamin D effects dependent on concentration
The effects of vitamin D in the organism are concentration- and tissue-dependent [65], and primarily mediated by calcitriol ( 1,25(OH)2 D3 ). However, the gold standard for determining vitamin D status are the more constant calcidiol plasma levels ( 25(OH)D3 ), which are measurable easier [71]. Calcidiol plasma levels are, however, not necessarily correlated with calcitriol levels.
Calcidiol has a longer half-life than calcitriol (21 d– 30 d vs. 4 h–48 h) and is present in a 1000-fold higher concentration [37][60]. More than 99 % of calcidiol in blood is bound to transport proteins, such as vitamin D-binding protein (VDP, 85 %, high affinity ) or albumin (15 %, lower affinity) [8][10]. Mainly the unbound fraction (<< 1 %) is effective [8]. Thus, the transport proteins and the widespread VDP polymorphism also influence the vitamin D effect [10]. This may lead, for example, to a sufficient amount of biologically effective, free amount of calcitriol in serum despite a seeming calcidiol deficiency. In addition, the active level is finely regulated in tissues themselves by means of 1α-hydroxylases. Furthermore, the effects can be altered via the availability of vitamin D receptor (VDR) binding sites [14][15 ]. The low and spatially varying concentrations, different and insufficiently standardized analytical methods may lead to measurement based differences in calcidiol levels of over 38 % [39][60]. This must be taken into account when interpreting vitamin D values [57]. It also provides an explanation for the divergent study results and recommendations on vitamin D.
Estimating the “normal” requirement
As previously shown, there are large differences in literature regarding normative ranges for vitamin D values. The determination of normal vitamin D requirement is crucial to the question of whether and how much vitamin D should be supplemented. The German Robert Koch Institute and other internationally renowned institutions use the classification of the US Institute of Medicine [45] to assess the vitamin D status. According to this classification, a vitamin D deficiency exists if calcidiol concentration is below 20 ng/ml (= 50 nmol/l). The current recommendations of the D-A-CH also mention 20 ng/ml (= 50 nmol/l) as a threshold value [19]. This serum level is based on the occurrence of deficiency symptoms such as rickets and other skeletal diseases.
However, more recent epidemiological studies make the case for a significantly higher normative range. Vitamin D serum concentrations above 30 ng/ml (= 75 nmol/l) reduce cardiometabolic and inflammatory biomarkers and lower morbidity for metabolic syndrome (MetS), diabetes , and cardiometabolic diseases [26]. The serum calcidiol levels of indigenous ethnic groups living close to the equator are even twice as high as the IOM recommendations. Among the traditionally living Hadzabe and Maasai in Tanzania (“model ethnic groups”), an average of 46 ng/ml (= 115 nmol/l) was measured [ 41]. The available epidemiological data as well as the serum levels of ethnic groups living close to the equator suggest that the vitamin D standard value ranges should be raised.
Vitamin D deficiency in the population
Due to its rather unspecific symptoms such as adynamia, susceptibility to infections, reduced muscle strength, myalgia, neurological disorders, orthostatic dysregulation, and skeletal complaints, vitamin D deficiency usually remains undetected [5]. In Germany, about 30 % of adults have a calcidiol level below 12 ng/ml (= 30 nmol/l). About 1/3 of German men and women exhibit concentrations between 12 ng/ml (= 30 nmol/l ) and 20 ng/ml (= 50 nmol/l) [56]. This means that the vast majority of the German population (> 60 %) has an undersupply of vitamin D. In Europe, about 40 % of the population has a serum calcidiol level below 20 ng/ml (= 50 nmol/l) [16]. The main reasons for the undersupply are insufficient dietary vitamin D intake and reduced vitamin D production via skin. Figure 2 shows the main factors influencing vitamin D levels.
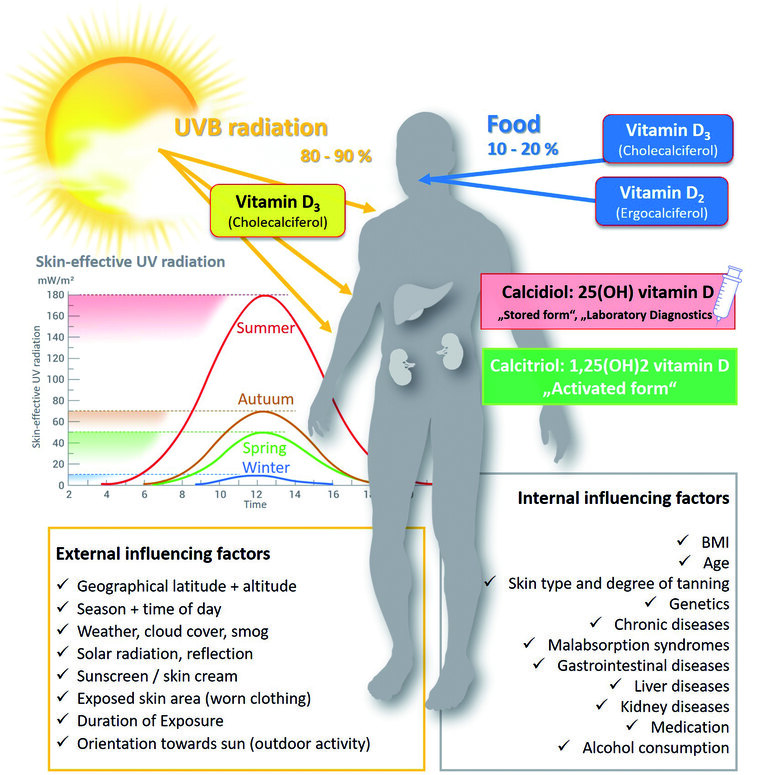
Figure 2: Physiologically active forms of vitamin D and factors influencing vitamin D levels
Nutrition
Only a small part (up to roughly 20 %) of the required amount of vitamin D can be obtained from dietary intake [52]. This is due to the fact that only a few, almost exclusively animal-based foods contain significant amounts of vitamin D [33]. Vegetarians and vegans therefore have an increased risk of undersupply. Vitamin D is mainly found in fatty sea fish (herring: 7.8—25 μg/100 g, salmon: 16 μg/100 g), chicken eggs (2.9 μg/100 g). Trace amounts can be found in dairy products and animal liver. Fungi and lichens can produce high concentrations of vitamin D2 (ergocalciferol) under UV irradiation, which is, however, less effective compared to vitamin D3 [34][40 ][66].
The D-A-CH now recommends a daily vitamin D intake of 800 IU (= 20 µg) for adults [71]. According to the National Nutrition Survey II [46], over 80 % of men and over 90 % of women do not reach the daily recommended vitamin D intake. Among senior citizens, this figure rises to over 95 %.
Vitamin D production in the skin
The main source of vitamin D is endogenous synthesis, which takes place in the human skin under influence of UVB radiation from the sun which depends on a variety of factors [23] such as sun position ( geographical latitude, season, time of day, altitude), environmental factors (smog/ weather, shade or surface reflection of the environment), skin type, and age [23][68]. Some of these factors that can be influenced, including exposed skin area, time of day, use of sunscreen/skin creams, duration of exposure, but also body fat percentage [69]. Sunburn should be avoided in any case because of the increased risk of skin cancer.
According to the Federal Office for Radiation Protection [11], sunbathing of uncovered face, hands, and arms (without sunscreen) for 12 minutes 2 to 3 times a week leads to a sufficient vitamin D production in the skin. These recommendations apply to a UV index of 7, which is usually reached in Germany under good weather conditions only and around midday during the months of June and July [13]. In the remaining summer months however, a much longer exposure is necessary due to lower UV indices. In the winter half-year (October to March), UVB radiation in Germany is too low for sufficient vitamin D production [12]. With regards to the vitamin D levels stated above, it is obvious that the vitamin D supplies stored in fat, muscle tissue, and liver are insufficient to compensate for the reduced UVB radiation for 6 months. The typical wave-shaped annual course of vitamin D levels for residents in Germany is shown in Figure 3 .
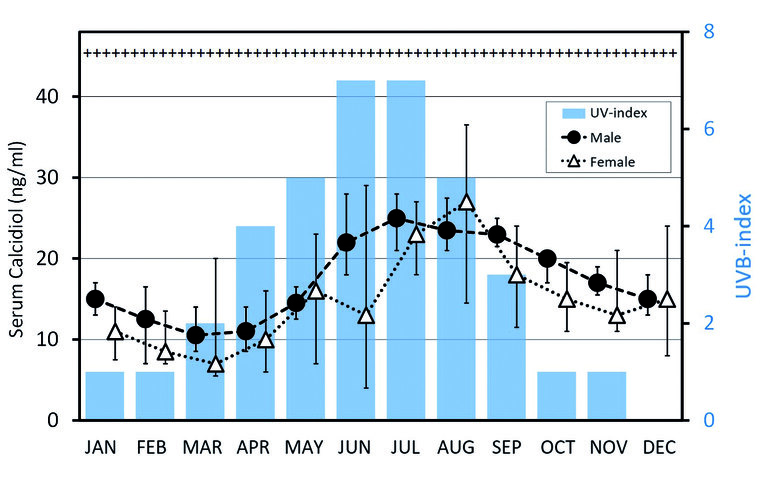
Figure 3: Typical seasonal course of vitamin D serum levels [24] and UVB indices (bar chart) [12] in Germany. The physiological levels of vitamin D in indigenous ethnic groups living close to the equator never drop below 40ng/ml (> 100 nmol/l) [41]and are marked with +++.
Population groups with increased vitamin D requirements
It is obvious that people with dark skin, vegetarians, and vegans are at an increased risk of vitamin D deficiency. Elderly (especially immobile) people, infants, young children , and pregnant women are also among the risk groups. Overweight , obesity [50], dental periodontitis, numerous diseases as well as certain medical drugs can have a negative impact on vitamin D levels. Table 1 provides an overview of the corresponding drugs and diseases.
Living environments
The problem of an adequate vitamin D supply is further exacerbated by modern lifestyles and changes in lifestyles. When staying in closed rooms, behind glass, and in vehicles, UVB exposure is de facto almost nil – even in sunshine. However, merely spending time outdoors does not guarantee sufficient vitamin D production, as UVB radiation in the morning and evening hours is only a fraction of the radiation during midday. People who do not work outdoors and shift workers are therefore particularly often affected by a deficiency [17 ]. In addition, when spending time outdoors, considerable areas of skin are usually covered by lotions, sunscreen, and clothing and thus insufficiently involved in vitamin D production. For example, a sunscreen with an UV protection factor of 8 reduces vitamin D synthesis by 93 % [71].
Female and male soldiers
In the military, the wearing of uniforms, protective equipment, and headgear as well as indoor activities, and staying in air, land and water vehicles lead to a significant restriction of endogenous vitamin D production. Therefore, a widespread and often unrecognised vitamin D deficiency in soldiers may be assumed. So far, current figures on vitamin D supply in the Bundeswehr are only available from a small and non-representative collective of 2176 pilots and aircrew. Of these, 71.6 % showed vitamin D deficiencies [55].
In contrast to the civilian sector, vitamin D may be even more important in military, police, and fire services. Due to high additional loads caused by protective clothing, equipment, and armament, duty related activities may lead to acute or persisting situations with significantly increased risks of stress fractures, among other things, especially if a vitamin D deficiency exists [ 18]. This is even more relevant for female soldiers [47].
Conclusion and recommendation
A high vitamin D level provides numerous health benefits. More and more professional organisations recommend vitamin D supplementation, ranging from 800 IU (= 20 µg) to 10,000 IU (= 250 µg). In some countries (USA, Canada, India and Finland), foods such as milk, yoghurt, and orange juice are already enriched with vitamin D [52].
Although there is no representative data on vitamin D levels in Bundeswehr soldiers, a widespread vitamin D deficiency among male and female soldiers is highly likely, especially throughout the winter half-year. Therefore, targeted supplementation with vitamin D seems to be appropriate. Studies with soldiers from other nations show that daily doses of 2000 IU/d (= 50 µg/d) vitamin D in combination with calcium lead to an improvement in bone health and a decrease in fracture rates [64]. The recently published systematic review “Nonexercise interventions for prevention of musculoskeletal injuries in armed forces ” also confirms a preventive effect of vitamin D, calcium and protein supplementation [6].
A common argument against vitamin D supplementation is the risk of overdosing. However, hypervitaminosis with vitamin D is very rare. An elevated risk exists primarily in the presence of an idiopathic infantile hypercalcemia [62], which can, however , be easily diagnosed in suspected cases by determining the 24,25 : 25 vitamin D metabolite ratio in the blood [4 ]. Hypervitaminoses in healthy individuals normally occur only in case of massive overdosing, such as in daily amounts exceeding 50,000 IU (= 1,250 µg/d), usually over months or years [25 ]. There, toxic serum concentrations measured ranged from 150 ng/ml to 1,220 ng/ml (= 375 nmol/l–3,050 nmol/ l) [25]. In case of suspicion, hypervitaminosis can be easily detected and prevented by determination of vitamin D levels.
In view of the current state of studies and the specific demands of the military sector, a targeted supplementation of vitamin D for soldiers is clearly recommended.
References
- Abdi F, Amjadi MA, Zaheri F, Rahnemaei FA: Role of vitamin D and calcium in the relief of primary dysmenorrhea: a systematic review. Obstet Gynecol Sci 2021; 64 (1): 13-26. mehr lesen
- Abdi F, Ozgoli G, Rahnemaie FS: A systematic review of the role of vitamin D and calcium in premenstrual syndrome. Obstet Gynecol Sci 2019; 62 (2): 73-86. mehr lesen
- Acipinar S, Karsiyaka Hendek M, Olgun E, Kisa U: Evaluation of FGF-23 and 25(OH)D3 levels in peri-implant sulcus fluid in peri-implant health and diseases. Clin Implant Dent Relat Res 2019; 21 (5): 1106-1112. mehr lesen
- Amrein K, Scherkl M, Hoffmann M et al.: Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr 2020; 74 (11): 1498-1513. mehr lesen
- Aoun A, Maalouf J, Fahed M, El Jabbour F: When and How to Diagnose and Treat Vitamin D Deficiency in Adults: A Practical and Clinical Update. J Diet Suppl 2020; 17 (3): 336-354. mehr lesen
- Arslan IG, Dijksma I, van Etten-Jamaludin FS, Lucas C, Stuiver MM: Nonexercise interventions for prevention of musculoskeletal injuries in armed forces: A systematic review and meta-analysis. Am J Prev Med 2021; 60 (2): e73-e84. mehr lesen
- Autier P, Mullie P, Macacu A et al.: Effect of vitamin D supplementation on non-skeletal disorders: a systematic review of meta-analyses and randomised trials. Lancet Diabetes Endocrinol 2017; 5 (12): 986-1004. mehr lesen
- Bikle DD, Schwartz J: Vitamin D binding protein, total and free Vitamin D levels in different physiological and pathophysiological conditions. Front Endocrinol (Lausanne) 2019; 10: 317. mehr lesen
- Botelho J, Machado V, Proença L, Delgado AS, Mendes JJ: Vitamin D deficiency and oral health: A comprehensive review. Nutrients 2020; 12 (5): 1471. mehr lesen
- Bouillon R, Schuit F, Antonio L, Rastinejad F: Vitamin D binding protein: A historic overview. Front Endocrinol (Lausanne) 2019; 10: 910. mehr lesen
- Bundesamt für Strahlenschutz: Konsentierte Empfehlung zu UV-Strahlung und Vitamin D.
- Bundesamt für Strahlenschutz: UV-Index weltweit.
- Bundesamt für Strahlenschutz: UV-Prognose.< https://www.bfs.de/DE/themen/opt/uv/uv-index/prognose/prognose_node.html)>, last access on June 9, 2021. mehr lesen
- Carlberg C: Nutrigenomics of Vitamin D. Nutrients 2019; 11 (3): 676. mehr lesen
- Carlberg C, Haq A: The concept of the personal vitamin D response index. J Steroid Biochem Mol Biol 2018; 175: 12-17. mehr lesen
- Cashman KD, Dowling KG, Škrabáková Z et al.: Vitamin D deficiency in Europe: pandemic? Am J Clin Nutr 2016; 103 (4): 1033-1044. mehr lesen
- Coppeta L, Papa F, Magrini A: Are shiftwork and indoor work related to D3 Vitamin deficiency? A systematic review of current evidences. J Environ Public Health 2018; 2018: 8468742. mehr lesen
- Dao D, Sodhi S, Tabasinejad R et al.: Serum 25-Hydroxyvitamin D levels and stress fractures in military personnel: A systematic review and meta-analysis. Am J Sports Med 2015; 43 (8): 2064-2072. mehr lesen
- Deutsche Gesellschaft für Ernährung e. V.: Referenzwerte Vitamin D (Calciferole).
- Deutsche Gesellschaft für Ernährung e. V.: Vitamin D und COVID-19.
- Dietrich T, Joshipura KJ, Dawson-Hughes B, Bischoff-Ferrari HA: Association between serum concentrations of 25-hydroxyvitamin D3 and periodontal disease in the US population. Am J Clin Nutr 2004; 80 (1): 108-113. mehr lesen
- Dusso AS, Brown AJ, Slatopolsky E: Vitamin D. Am J Physiol Renal Physiol 2005; 289 (1): F8-28. mehr lesen
- Engelsen O: The relationship between ultraviolet radiation exposure and vitamin D status. Nutrients 2010; 2 (5): 482-495. mehr lesen
- Francic V, Keppel M, Schwetz V et al.: Are soluble ST2 levels influenced by vitamin D and/or the seasons? Endocr Connect 2019; 8 (6): 691-700. mehr lesen
- Galior K, Grebe S, Singh R: Development of Vitamin D toxicity from overcorrection of Vitamin D deficiency: A review of case reports. Nutrients 2018; 10 (8): 953. mehr lesen
- Ganji V, Tangpricha V, Zhang X: Serum Vitamin D Concentration ≥75 nmol/l Is Related to Decreased Cardiometabolic and Inflammatory Biomarkers, Metabolic Syndrome, and Diabetes; and Increased Cardiorespiratory Fitness in US Adults. Nutrients 2020; 12 (3): 730. mehr lesen
- Gao W, Tang H, Wang D et al.: Effect of short-term vitamin D supplementation after nonsurgical periodontal treatment: A randomized, double-masked, placebo-controlled clinical trial. J Periodontal Res 2020; 55 (3): 354-362. mehr lesen
- Ghorbani Z, Togha M, Rafiee P et al.: Vitamin D in migraine headache: a comprehensive review on literature. Neurol Sci 2019; 40 (12): 2459-2477. mehr lesen
- Gregoriou E, Mamais I, Tzanetakou I, Lavranos G, Chrysostomou S: The effects of Vitamin D supplementation in newly diagnosed type 1 diabetes tatients: systematic review of randomized controlled trials. Rev Diabet Stud 2017; 14 (2-3): 260-268. mehr lesen
- Guan Y, Hao Y, Guan Y, Bu H, Wang H: The effect of Vitamin D supplementation on rheumatoid arthritis patients: A systematic review and meta-analysis. Front Med (Lausanne) 2020; 7: 596007. mehr lesen
- Holick MF: Vitamin D deficiency. N Engl J Med 2007; 357 (3): 266-281. mehr lesen
- Holick MF, Binkley NC, Bischoff-Ferrari HA et al.: Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2011; 96 (7): 1911-1930. mehr lesen
- Holick MF, Chen TC: Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr 2008; 87 (4): 1080S-1086S. mehr lesen
- Houghton LA, Vieth R: The case against ergocalciferol (vitamin D2) as a vitamin supplement. Am J Clin Nutr 2006; 84 (4): 694-697. mehr lesen
- Jolliffe DA, Camargo CA, Sluyter JD et al.: Vitamin D supplementation to prevent acute respiratory infections: systematic review and meta-analysis of aggregate data from randomised controlled trials. Lancet 2021; 9 (5):276-292. mehr lesen
- Kazemi A, Mohammadi V, Aghababaee SK et al.: Association of Vitamin D status with SARS-CoV-2 infection or COVID-19 severity: A systematic review and meta-analysis. Adv Nutr 2021; nmab012 [Online ahead of print]. mehr lesen
- Kennedy DA, Cooley K, Skidmore B et al.: Vitamin d: pharmacokinetics and safety when used in conjunction with the pharmaceutical drugs used in cancer patients: a systematic review. Cancers (Basel) 2013; 5 (1): 255-280 mehr lesen
- Keum N, Lee DH, Greenwood DC, Manson JE, Giovannucci E: Vitamin D supplementation and total cancer incidence and mortality: a meta-analysis of randomized controlled trials. Ann Oncol 2019; 30 (5): 733-743 mehr lesen
- Lips P, Chapuy MC, Dawson-Hughes B, Pols HA, Holick MF: An international comparison of serum 25-hydroxyvitamin D measurements. Osteoporos Int 1999; 9 (5): 394-397 mehr lesen
- Logan VF, Gray AR, Peddie MC, Harper MJ, Houghton LA: Long-term vitamin D3 supplementation is more effective than vitamin D2 in maintaining serum 25-hydroxyvitamin D status over the winter months. Br J Nutr 2013; 109 (6): 1082-1088. mehr lesen
- Luxwolda MF, Kuipers RS, Kema IP, Dijck-Brouwer DAJ, Muskiet FAJ: Traditionally living populations in East Africa have a mean serum 25-hydroxyvitamin D concentration of 115 nmol/l. Br J Nutr 2012; 108 (9): 1557-1561. mehr lesen
- Machado V, Lobo S, Proença L, Mendes JJ, Botelho J: Vitamin D and periodontitis: A systematic review and meta-analysis. Nutrients 2020; 12 (8): 12(8): 2177. mehr lesen
- Mansourian M, Rafie N, Khorvash F, Hadi A, Arab A: Are serum vitamin D, calcium and phosphorous associated with restless leg syndrome? A systematic review and meta-analysis. Sleep Med 2020; 75: 326-334. mehr lesen
- Maretzke F, Bechthold A, Egert S et al.: Role of Vitamin D in preventing and treating selected extraskeletal diseases-An umbrella review. Nutrients 2020; 12(4): 969. mehr lesen
- National Institutes of Health: Vitamin D. Sheet for health professionals.
- Nationale Verzehrsstudie II. Ergebnisbericht Teil 2. Karlsruhe, 2008. mehr lesen
- Nestler K, Tofaute KA, Leyk D: Frauen in der Bundeswehr. Wehrmed Wehrpharm 2016; 16 (4): 99-101. mehr lesen
- New reference values for vitamin D. Ann Nutr Metab 2012; 60 (4): 241-246. mehr lesen
- Niedermaier T, Gredner T, Kuznia S et al.: Vitamin D supplementation to the older adult population in Germany has the cost-saving potential of preventing almost 30 000 cancer deaths per year. Mol Oncol 2021; [Online ahead of print]. mehr lesen
- Oliveira LF de, Azevedo LG de, Da Mota Santana J, de Sales, Luanna Pimenta Carlos, Pereira-Santos M: Obesity and overweight decreases the effect of vitamin D supplementation in adults: systematic review and meta-analysis of randomized controlled trials. Rev Endocr Metab Disord 2020; 21 (1): 67-76. mehr lesen
- Perayil J, Menon KS, Kurup S et al.: Influence of Vitamin D & Calcium supplementation in the management of periodontitis. J Clin Diagn Res 2015; 9 (6): ZC35-8. mehr lesen
- Pilz S, März W, Cashman KD et al.: Rationale and plan for Vitamin D food fortification: A review and guidance paper. Front Endocrinol (Lausanne) 2018; 9: 373. mehr lesen
- Pilz S, Zittermann A, Trummer C et al.: Vitamin D testing and treatment: a narrative review of current evidence. Endocr Connect 2019; 8 (2): R27-R43. mehr lesen
- Pilz, S et al.: Vitamin D and mortality Anticancer Res 2016 (36): 1379-1388. mehr lesen
- Pippig T, Matthias O, Zahedi F: Erste Ergebnisse: Vitamin-D-Versorgung bei Piloten und Luftfahrtpersonal der Bundeswehr. Flug u Reisemed 2019; 26 (04): 171-178. mehr lesen
- Rabenberg M, Scheidt-Nave C, Busch MA et al.: Vitamin D status among adults in Germany--results from the German Health Interview and Examination Survey for Adults (DEGS1). BMC Public Health 2015; 15: 641. mehr lesen
- Rabenberg M, Scheidt-Nave C, Busch MA et al.: Implications of standardization of serum 25-hydroxyvitamin D data for the evaluation of vitamin D status in Germany, including a temporal analysis. BMC Public Health 2018; 18 (1): 845. mehr lesen
- Ramasamy I: Vitamin D metabolism and guidelines for Vitamin D supplementation. Clin Biochem Rev 2020; 41 (3): 103-126. mehr lesen
- Robien K, Oppeneer SJ, Kelly JA, Hamilton-Reeves JM: Drug-vitamin D interactions: a systematic review of the literature. Nutr Clin Pract 2013; 28 (2): 194-208. mehr lesen
- Romagnoli E, Pepe J, Piemonte S, Cipriani C, Minisola S: Management of endocrine disease: value and limitations of assessing vitamin D nutritional status and advised levels of vitamin D supplementation. Eur J Endocrinol 2013; 169 (4): R59-69. mehr lesen
- Ross AC, Taylor CL, Yaktine AL, Del Valle HB (ed.): Dietary reference intakes for Calcium and Vitamin D. Washington (DC): National Academies Press 2011. mehr lesen
- Schlingmann KP, Kaufmann M, Weber S et al.: Mutations in CYP24A1 and idiopathic infantile hypercalcemia. N Engl J Med 2011; 365 (5): 410-421. mehr lesen
- Scientific Advisory Committee on Nutrition: Vitamin D and health report.
- Sivakumar G, Koziarz A, Farrokhyar F: Vitamin D supplementation in military personnel: A systematic review of randomized controlled trials. Sports Health 2019; 11 (5): 425-431. mehr lesen
- Spedding S, Vanlint S, Morris H, Scragg R: Does vitamin D sufficiency equate to a single serum 25-hydroxyvitamin D level or are different levels required for non-skeletal diseases? Nutrients 2013; 5 (12): 5127-5139. mehr lesen
- Tripkovic L, Wilson LR, Hart K et al.: Daily supplementation with 15 μg vitamin D2 compared with vitamin D3 to increase wintertime 25-hydroxyvitamin D status in healthy South Asian and white European women: a 12-wk randomized, placebo-controlled food-fortification trial. Am J Clin Nutr 2017; 106 (2): 481-490. mehr lesen
- VitaminD Society: The VitaminD Society.
- Webb AR: Who, what, where and when-influences on cutaneous vitamin D synthesis. Prog Biophys Mol Biol 2006; 92 (1): 17-25. mehr lesen
- Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF: Decreased bioavailability of vitamin D in obesity. Am J Clin Nutr 2000; 72 (3): 690-693. mehr lesen
- Zhou F, Zhou Y, Shi J: The association between serum 25-hydroxyvitamin D levels and dental caries in US adults. Oral Dis 2020; 26 (7): 1537-1547. mehr lesen
- Zittermann A, Pilz S: Vitamin D in Klinik und Praxis. Dtsch Med Wochenschr 2017; 142 (8): 601-616. mehr lesen
Manuscript Data
Submitted : June 3, 2021
Accepted : June 25, 2021
Citation
Vits E, Staudt M, Berresheim M, Rohde U, Eger T, Bickel C, Leyk D: Vitamin D deficiency: An often underestimated risk. WMM 2021; 65(8): 308–314.
For the authors
Major (MC) Dr. Emanuel Vits
Bundeswehr Institute for Preventive Medizin
Division A – Health and Fitness Promotion
Andernacher Str. 100; D-56070 Koblenz
E-Mail: emanuelvits@bundeswehr.org