AEROMEDICAL RISK ASSESSMENT
Case report: An incidental finding of a cerebellar parenchymal lesion in a pilot candidate during the initial assessment of fitness for military flying duties
Josef Ehlinga,b, Sven-Erik Sönksena, Daniel A. Veitb, Stephan Waldeckb, Hans-Jürgen Nobléa
a Air Force Centre of Aerospace Medicine, Section II 3 g – Diagnostic Imaging, Fürstenfeldbruck, Germany
b Bundeswehr Central Hospital, Department VIII – Radiology and Neuroradiology, Koblenz, Germany
Abstract
In this case report, we demonstrate the utility of modern imaging modalities in the medical assessment of fitness for military flying duties at the German Air Force Centre of Aerospace Medicine. We report the rare case of a 27-year-old pilot candidate with a functionally compensated cerebellar lesion that occurred in early childhood. Contrast-enhanced 3 Tesla magnetic resonance imaging and magnetic resonance spectroscopy revealed a cerebellar structural abnormality characteristic of a degenerative cystic parenchymal lesion. Imaging ruled out ischaemic and haemorrhagic processes, hamartomatous overgrowth (dysplastic gangliocytoma of the cerebellum or Lhermitte-Duclos disease), and malignant processes. Based on these findings, the lesion was assessed as unlikely to adversely affect the applicant’s long-term fitness for military flying duties.
Keywords: radiology, magnetic resonance imaging, pilot candidate, fitness for flying duties, Lhermitte-Duclos disease, low-grade glioma
Background
Military pilots must meet particularly high demands when it comes to their cognitive and motor skills under extreme conditions. For this reason, acute or chronic diseases of the central nervous system play an important role in aeromedical assessments at the German Air Force Centre of Aerospace Medicine.
All applicants for the flying service of the Bundeswehr (German Armed Forces) must undergo an interdisciplinary assessment of their fitness for military flying duties at the German Air Force Centre of Aerospace Medicine. This includes non-invasive imaging. Magnetic resonance imaging (MRI) at 3 Tesla (3T) is performed in order to rule out or assess structural lesions of the central nervous system (CNS) which are of aeromedical relevance. MRI-based screening includes a scan of the whole spine and a multi-sequence 3D scan of the neurocranium. [ 6]
Diagnostic imaging is conducted at the Air Force Centre of Aerospace Medicine prior to the beginning of flight training in order to rule out the presence of conditions of aeromedical relevance or variants that are associated with an unfavourable prognosis and an increased risk of the feared case of what is known as sudden incapacitation of the pilot. Examples include intracranial arteriovenous malformation or intradural aneurysms associated with an increased lifetime prevalence of intracranial haemorrhage, cerebrospinal fluid flow obstruction, intra-axial masses, and inflammatory white-matter lesions.
Case presentation
History
A 27-year-old male soldier and student of sports science applied for a career as a pilot of fixed-wing aircraft in the flying service of the Bundeswehr. During his previous training as a sports officer, no cognitive or motor deficits had been noted. He successfully completed an aptitude assessment and achieved above-average results in the initial psychological assessment. He reported good subjective health when he presented to the Air Force Centre of Aerospace Medicine in Fürstenfeldbruck for an aeromedical assessment of his fitness for military flying duties.
Magnetic resonance imaging
Every applicant for the flying service of the Bundeswehr undergoes an assessment of his or her fitness for military flying duties at the German Air Force Centre of Aerospace Medicine. This assessment includes routine non -enhanced magnetic resonance imaging (MRI) of the neurocranium and the entire axial skeleton at a field strength of 3 Tesla . [6]
In the case of the 27-year-old pilot candidate, MRI revealed a right cerebellar spongy and cystic transformation zone that involved the anterior cortex and white matter and extended to the cerebellar vermis. The transformation zone measured 2.7 x 3.1 x 3.1 cm (RL x CC x AP ) and was hyperintense on T2-weighted images. There was no mass effect and no surrounding oedema (Figs. 1 A – H ).
After the applicant’s written informed consent had been obtained , an additional MRI scan with intravenous contrast was performed in order to further assess these unusual cerebellar findings. Following intravenous administration of a cyclic gadolinium-based contrast agent, no abnormal contrast enhancement indicative of a blood-brain barrier disorder was detected (Figs. 1 I – J).
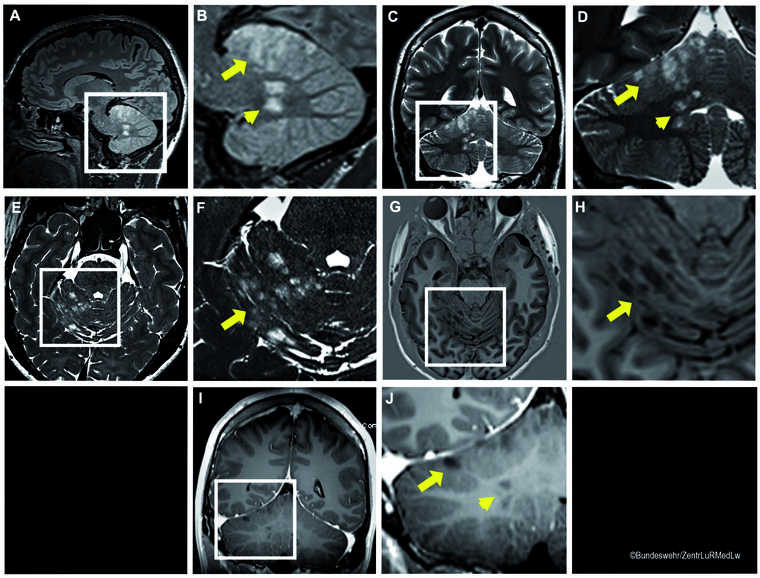
Figure 1. MRI during the initial assessment of the applicant’s fitness for military flying duties
Non-contrast-enhanced MRI (a – h) demonstrated a spongy and cystic T2-hyperintense and T1-hypointense transformation zone involving the cortex (arrows) and white matter (arrowheads) of the right cerebellar hemisphere.
After intravenous contrast agent administration (i – j), there was no evidence of a blood-brain barrier disorder.
MRI sequences:
A – B) sagittal T2 dark fluid, C – D) coronal T2 TSE, E – F) transverse thin-slice T2 SPACE, G – H) transverse T1 IR, I – J) post-contrast coronal T1 fl2d
Specific MRI sequences that are used to detect ischaemia or haemorrhage and to evaluate blood vessels were also performed in order to rule out an ischaemic or haemorrhagic cause (Figs. 2 A – H). Neither diffusion-weighted imaging (Figs . 2 A – D) nor susceptibility-weighted imaging (SWI) (Figs. 2 E – F) revealed abnormalities suggestive of infarction or haemorrhage. Vertebrobasilar dissection and the absence of blood flow in the superior cerebellar artery were ruled out by time-of-flight (TOF ) angiography (Figs. 2 G – H). Since the parenchymal lesion was located both in right cerebellar white matter and the cortex and involved areas supplied by the superior cerebellar artery, it was of crucial importance to rule out a haemorrhagic or ischaemic cause in the aeromedical assessment.
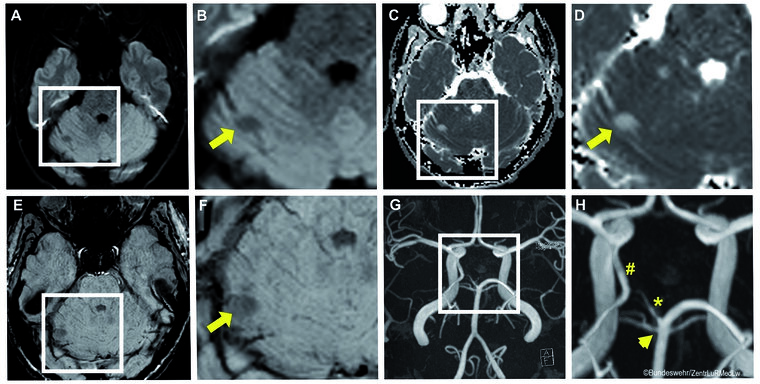
Figure 2. Specific MRI sequences for the detection of ischaemia or haemorrhage and the evaluation of blood vessels
There was no evidence of an ischaemic aetiology of the right-sided spongy and cystic lesion of the cerebellum (arrows) with a nonspecific loss of signal on diffusion-weighted sequences (A – B) and T2 shine through on apparent diffusion coefficient (ADC) maps (C – D). In addition, there was nonspecific low signal intensity on SWI MIP sequences, which provided no evidence of past (micro)bleeds (E – F).
Non-contrast-enhanced 3D TOF angiography (MIP) showed a normal origin of the right superior cerebellar artery (arrowhead) and the absence of vertebrobasilar dissection (G – H). An additional finding was an anatomical variant, i.e. a foetal origin of the right posterior cerebral artery from the internal carotid artery (#) with a hypoplastic P1 segment of the right posterior cerebral artery (*).
Additional findings were a cystic transformation of the pineal gland (measuring approximately 0.6 x 1.1 cm) without a mass effect and a small spindle-shaped left temporopolar arachnoid cyst (measuring approximately 1.6 x 0.7 cm). Otherwise the neurocranium appeared normal in morphology.
Magnetic resonance spectroscopy
For a further diagnostic evaluation of the incidental neuroradiological findings, magnetic resonance spectroscopy (MRS) using a single-voxel technique was performed at the Department of Radiology and Neuroradiology of the Bundeswehr Central Hospital in Koblenz. This technique allows tissue to be assessed non -invasively for the presence and concentrations of different metabolites. Spectra are then compared to those of healthy brain parenchyma. For example, MRS is used to determine the concentrations of trimethylamine such as choline (Cho) as a marker of membrane phospholipid metabolism, creatine (Cr) as a marker of energy metabolism, and N-acetylaspartate (NAA) as a marker of the synthesis or breakdown of neuron-specific amino acid derivatives. [1][2][7 ] In addition, elevated concentrations of pathological metabolites may suggest an underlying malignancy. For example, this applies to an increase in lactate levels which reflects a switch from aerobic to anaerobic glycolysis. The presence of lipid peaks is indicative of tissue necrosis or metastasis. [7][8] Abnormal MRS spectra can thus provide evidence of nonspecific gliotic, acute inflammatory, necrotic, or proliferative changes.
Single-voxel spectroscopy (SVS) of the right cerebellar lesions of the 27-year-old pilot candidate showed a global decrease in choline (Cho), creatine (Cr) and N-acetylaspartate (NAA ). The NAA/Cr ratio was almost identical to that of the healthy white matter of the left cerebellar hemisphere (reference spectrum) (Fig. 3). There was neither an increase in the levels of pathological metabolites such as lipids or lactate nor an increase in the concentration of choline as a marker of cell proliferation (Fig. 3).
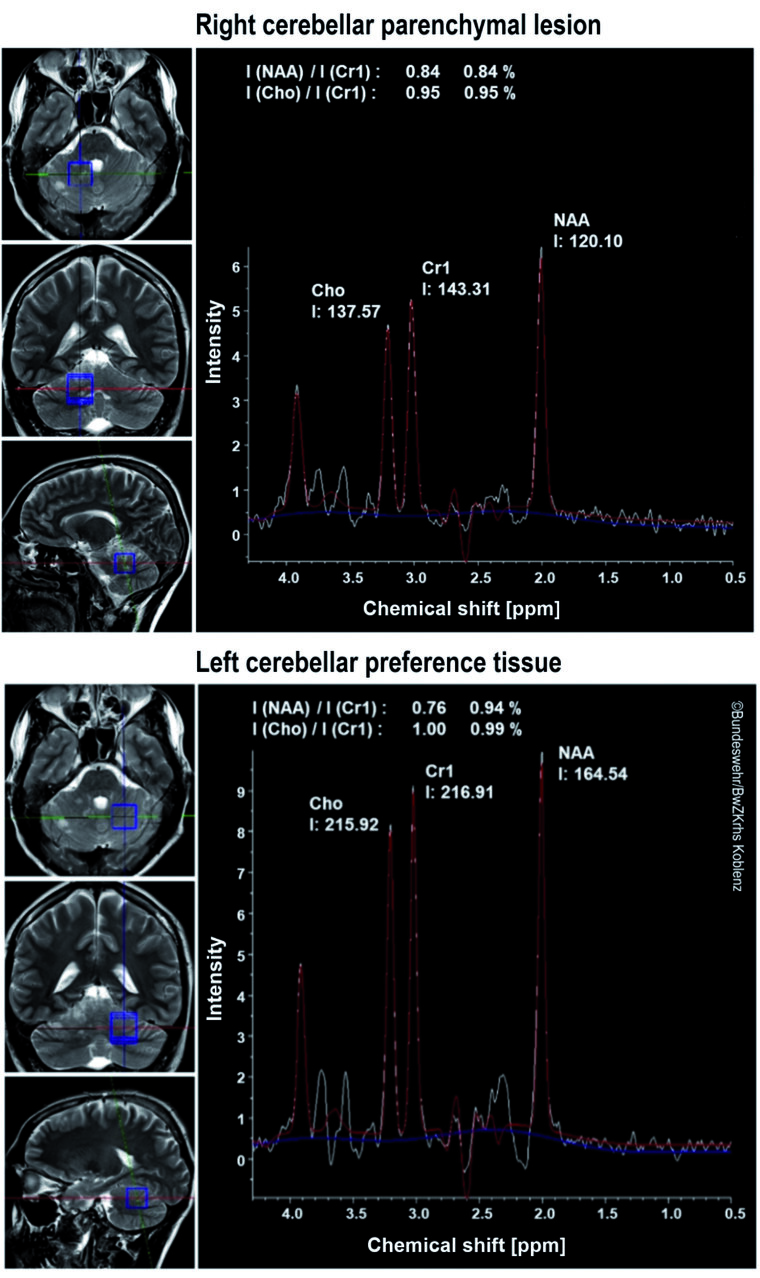
Figure 3. Magnetic resonance spectroscopy (MRS)
In the case presented here, single-voxel spectroscopy (SVS) of a representative right cerebellar white-matter lesion showed a decrease in choline (Cho), creatine (Cr) and N-acetylaspartate (NAA). The NAA/Cr ratio was almost identical to that of the healthy white matter of the left cerebellar hemisphere (reference spectrum) (I = integral).
In summary, magnetic resonance spectroscopy provided primary and robust evidence of a multi-focal right-sided cerebellar parenchymal lesion involving the cortex and white matter. MRS suggested a nonspecific neurodegenerative disease associated with multi-focal cerebellar gliosis without any evidence of proliferation. Consistent with these findings, the lesion showed no contrast enhancement and no mass effect on conventional MRI.
Discussion
Aeromedical assessment
On the basis of MRI and MRS findings, the parenchymal cerebellar lesion of the 27-year-old pilot candidate was considered to be a local circumscribed neurodegenerative lesion without any evidence of a proliferative process. Imaging studies ruled out an invasive intra-axial growth pattern and hamartomatous overgrowth (Lhermitte-Duclos disease). Ischaemic or haemorrhagic causes of the right cerebellar parenchymal lesion that was located in an area supplied by the superior cerebellar artery were ruled out as well.
An assessment of neurological function showed that the applicant had no neurological deficits. Future functional deficits are unlikely to result from this neurodegenerative parenchymal lesion , which was most probably acquired in early childhood. From an aeromedical perspective, the local circumscribed parenchymal lesion of the cerebellum has a favourable prognosis, on the basis of which the applicant can be assessed as fit for military flying duties and can be granted a special permit.
Differential diagnosis
Especially from a flight safety perspective, ischaemic and haemorrhagic causes must always be ruled out in the differential diagnosis of changes in the cortex and white matter of the cerebellum which involve areas supplied by the superior cerebellar artery. In addition, vertebrobasilar dissection is not an uncommon cause of infarction, particularly in young athletes, and must also be ruled out. [ 3]. Modern MRI techniques can systematically investigate these conditions in a rapid and non-invasive manner without requiring contrast agents. At the Air Force Centre of Aerospace Medicine, the standard protocol for the initial MRI-based assessment of applicants therefore includes specific MRI sequences that are used to detect ischaemia or haemorrhage and to evaluate blood vessels.
As a result of the spongy nature of the lesion, Lhermitte-Duclos disease and low-grade gliomas should also be considered in the differential diagnosis of cerebellar conditions such as those reported here. Lhermitte-Duclos disease is a variant of Cowden syndrome, which is a pleomorphic, autosomal dominant inherited condition and is clinically characterised by hamartomatous overgrowth affecting all three germ layers. Since the syndrome is associated with mutations in phosphatase and tensin homolog (PTEN, a tumour suppressor gene), it is one of several PTEN hamartoma tumour syndromes (PHTS). [4][9]
Clinically, Lhermitte- Duclos disease or dysplastic cerebellar gangliocytoma typically presents in adults with neurological symptoms that depend on the size of the cerebellar mass. Common clinical signs and symptoms of Lhermitte-Duclos disease are ataxia, increased intracranial pressure, and seizures caused by the cerebral hamartomatous tumour. Gangliocytomas are rarely associated with a PTEN mutation in children. [4][9]
Neuroradiological images of dysplastic gangliocytoma typically show widening of the cerebellar cortex with a striated appearance, usually of a cerebellar lobe, with T2 hyperintensity on MRI. Unlike a blood-brain barrier disorder, dysplastic cerebellar gangliocytoma is typically not associated with significant contrast enhancement.
MRS shows the decisive difference to (multi-focal) cerebellar gliosis. Dysplastic gangliocytoma or Lhermitte-Duclos disease is usually characterised by an increase in lactate levels, a decrease in the neuron-specific marker N-acetylaspartate (NAA), and a marked decrease in choline. By contrast, malignancies are associated with an increase in the concentration of choline (Cho) as a marker of cell proliferation. [ 5]
Since both Lhermitte-Duclos disease and low-grade gliomas can result in considerable functional impairment, they are disqualifying for military flying duties.
Conclusions
Modern diagnostic imaging modalities not only are useful in detecting conditions of aeromedical relevance in applicants for the flying service of the Bundeswehr but also allow findings to be characterised and assessed from an aeromedical perspective. Modern imaging techniques are thus particularly effective in evaluating abnormal findings on the basis of aeromedical aspects. These techniques can explicitly provide evidence that allows applicants with abnormal findings to be assessed as fit for flight training. Modern imaging is an effective tool in risk assessment and in differentiating more clearly between an anatomical variant with a favourable prognosis, a functionally compensated cerebellar condition that was acquired in early childhood, functionally significant brain damage, and a malformation that is associated with a poor prognosis.
Systematic MRI studies that are performed at the Air Force Centre of Aerospace Medicine in cooperation with the Department of Radiology and Neuroradiology at the Bundeswehr Central Hospital in Koblenz help not only to minimise the risk of the feared case of sudden incapacitation but also to satisfy personnel requirements, which is a particular challenge since the job of a military pilot is complex and demanding. As a result, this imaging approach has direct effects on the operational readiness of the armed forces. The case presented here shows that the use of modern imaging modalities in differential diagnosis and in the comprehensive evaluation of abnormal findings can increase the number of candidates who are assessed as fit for military flying duties. If regular MRI examinations are performed and the documented findings remain unchanged, special permits can be granted and long-term fitness for military flying duties can be guaranteed. This approach allows candidates with anatomical variations to be recruited and at the same time is fully consistent with the primacy of flight safety. The selection and recruitment of flight crew members must meet high requirements. In addition, flight crew training is time-consuming and cost- intensive. The special role of high-quality imaging in a well-considered aeromedical evaluation of findings becomes all the more evident when these aspects are taken into consideration.
Data protection declaration
The applicant agreed to the publication of medical findings from the initial assessment of fitness for military flying duties in an anonymised format and gave his written consent.
References
- Backens M: Technik der Protonen- und Phosphor-MR-Spektroskopie. Radiologe 2017; 57: 428–437. mehr lesen
- Bray MD, Mullins ME: Metabolic white matter diseases and the utility of MR spectroscopy. Radiol Clin 2014; 52: 403–411. mehr lesen
- De Cocker LJL, Lövblad K-O, Hendrikse J: MRI of cerebellar infarction. Eur Neurol 2017; 77(3-4): 137–146. mehr lesen
- Deutsche Gesellschaft für Kinderendokrinologie und -diabetologie (DGKED): Diagnostik und Management von Patienten mit PTEN Hamartom Tumor Syndrom (PHTS) im Kindes- und Jugendalter. DGKED 2019: Kapitel 2.5.
- Klisch J, Juengling F, Spreer J et al.: Lhermitte-Duclos disease: Assessment with MR Imaging, Positron Emission Tomography, Single-photon Emission CT, and MR Spectroscopy. AJNR Am J Neuroradiol 2001; 22(5): 824–830. mehr lesen
- Kommando Sanitätsdienst der Bundeswehr: Wehrfliegerverwendungsfähigkeit und weitere Tauglichkeitsbegutachtungen von Luftfahrtpersonal. KdoSanDstBw 2018; Zentralvorschrift A1-831/0-400: §§244 und 248.
- Lanfermann H, Herminghaus S, Pilatus U, Hattingen E, Zanella FE: Bedeutung der 1H-MR-Spektroskopie bei der Differenzialdiagnose und Graduierung intrakranieller Tumoren. Dtsch Arztebl 2004; 101: A 649–655. mehr lesen
- Reith W: MR-Spektroskopie in der klinischen Diagnostik. Radiologe 2017; 57: 427. mehr lesen
- Riegert-Johnson DL, Gleeson FC, Roberts M, et al: Cancer and Lhermitte-Duclos disease are common in Cowden syndrome patients. Hered Cancer Clin Pract 2010; 8(1): 6. mehr lesen
Manuscript data
Submitted : March 1, 2021
Accepted after revision: April 30, 2021
Citation
Ehling J, Sönksen SE , Veit DA, Waldeck S, Noblé HJ: Case report: An incidental finding of a cerebellar parenchymal lesion in a pilot candidate during the initial assessment of fitness for military flying duties. WMM 2021; 65(8): e315 – e319.
Corresponding author
Major (MC) Dr. Dr. Josef Ehling
Air Force Centre of Aerospace Medicine
Section II 3 g – Diagnostic Imaging
Straße der Luftwaffe 322, 82256 Fürstenfeldbruck, Germany
E-Mail: josef1ehling@bundeswehr.org